Gm Case 3
Case scenario:
Myself K. Pranay Kumarof 3rd bds . This is an online e log book to discuss our patient de-identified health data shared after taking her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio.
• Chief Complaint :-
A 67 years old female came to OPD with chief complaints of
-pedal edema since - 3months.
-Shortness of breath since - 3 months
- Decreased urine output since 3 months.
• History of present illness :-
Patient was apparently asymptomatic 1yr back then she noticed decreased urine output and was diagnosed to have heart failure and renal failure and started on conservative management.
Then 3months back she noticed increased Bilateral pedal edema -pitting type, extending till ankles .
shortness of breath - grade 3 insidious onset and progressive.
No history of burning micturition, paroxysmal nocturnal dyspnoea,cough, cold, fever.
• History of past illness :-
K/C/O Hypertension since 30 years, diabetes mellitus since 30 years
Not known case of asthma, tuberculosis, epilepsy.
• Medical history :-
For diabetes Tab Glimy 3mg/PO/BD.
For hypertension tab nicardia , Prolomet XL 50


• Personal history :-
Diet - Mixed
Appetite - Lost
Sleep - Adequate
Bowel and bladder movements- Irregular ( constipation)
Micturition - Abnormal
No addictions.
• Family history:-
No one of family has similar disease.
• General Examination :-
Patient is co-operative coherent consciousness and well oriented to place and time .
No pallor, cyanosis, icterus, lymphadenopathy, clubbing of fingers.
Edema - present
• Vitals : -
Temperature - 98 °F
Bp - 160/100 mmHg
Pulse rate - 100 bpm
Respiratory rate - 16 cycles/ min.
• Systemic Examination :-
Respiratory system -
Inspection : -
Chest is normal bilaterally symmetrical
Position of trachea is central
Movements are bilaterally symmetrical.
No scars , sinuses, or visible pulsations.
Suprasternal and supraclavicular notching is present.
Palpation :
No local rise of temperature
No tenderness
All inspectory findings are confirmed
Apex beat felt in 5th intercostal space 2cm lateral to midclavicular line .
Percussion :-
Resonant sound is heard
Auscultation
Normal vesicular sounds are heard.
CVS -
Inspection :
Bilaterally symmetrical chest
No visible engorged veins,scars or sinuses on chest.
Palpation :
S1 S2 are heard
No thrills , no murmurs
Apex beat present at 5th intercostal space 2cm lateral to midclavicular line .
Auscultation :
No cardiac murmurs heard.
Abdomen -
Obese, inverted umbilicus.
No visible scars, sinuses, fistulas, engorged veins.
No organomegaly.
Soft , non tender , no free fluid.
CNS -
Conscious, speech is normal, no neck stiffness and kernings sign negative.
No finger and nose in coordination.
Provisional diagnosis: - Chronic renal failure
HFpEF - Right heart failure.(Heart failure with preserved ejection fraction).
Investigations: -
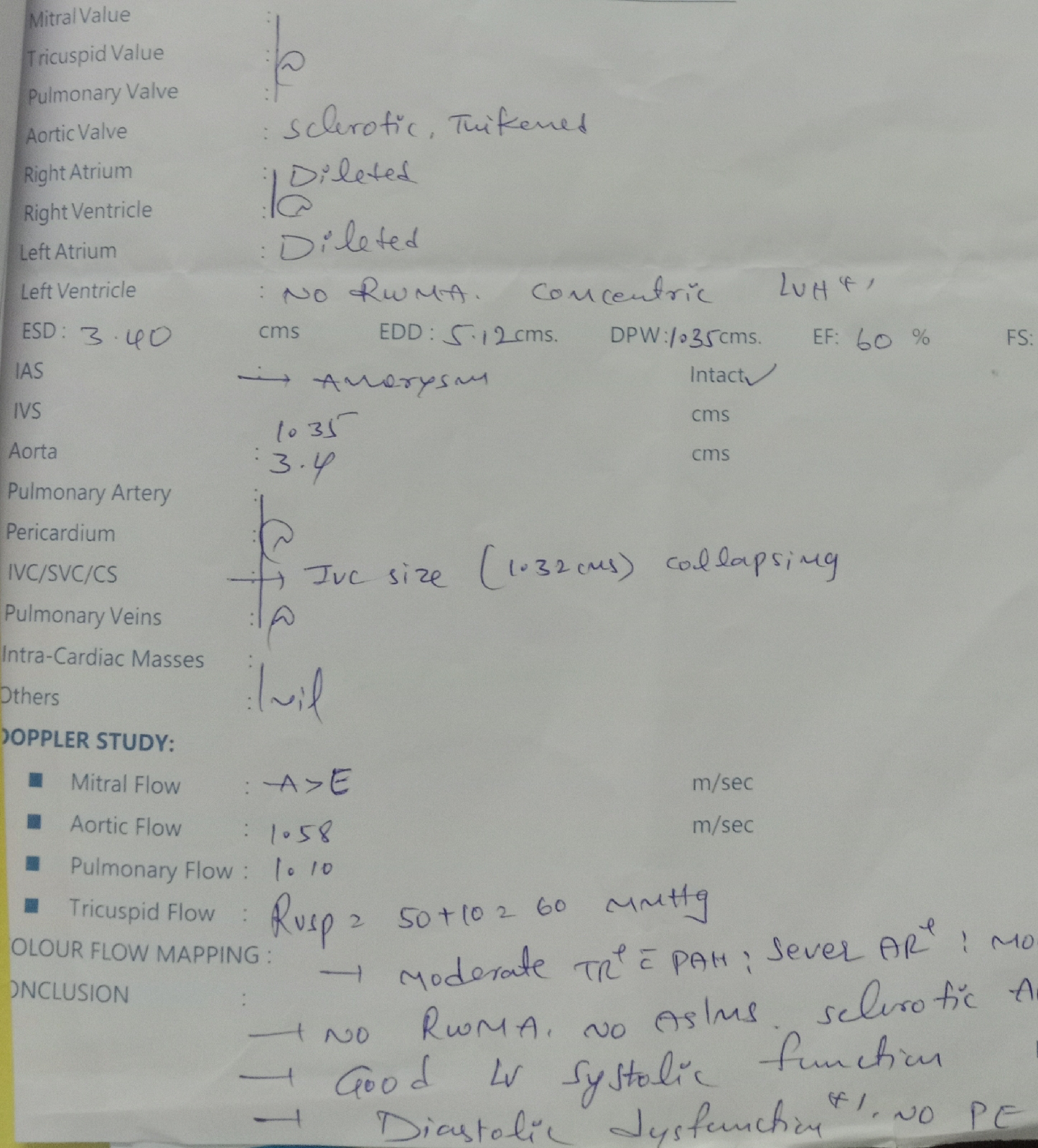
2D echo -
USG ABDOMEN :-

Complete Urine examination:-

Random Blood Sugar :-
Serum creatinine -
Serum electrolytes -

ECG -

Complete blood picture -




Tab Nodosis 500mg PO/BD
Tab shelcal PO/OD
Tab orofer XT PO/BD
Cap Bio D3 OD
Tab Nicardia 20mg PO/BD
Inj Erythropoietin 4000IU Once weekly




